

Journal Club - Tranexamic Acid in Trauma
/
https://www.maimonidesem.org/blog/txa-in-trauma
Background
Tranexamic acid (TXA), a lysine-derived synthetic agent, works by blocking the activation of plasminogen, thereby inhibiting fibrinolysis and stabilizing clots that have formed.[1]
The use of TXA in the care of the traumatically injured patient has become prevalent since the publication of the MATTERs and CRASH-2 studies which demonstrated significant mortality benefits in trauma patients who received early TXA after admission.[2][3] If earlier treatment with TXA is better, would there be benefit in its administration in the prehospital setting? If so, could this be done safely? These questions are asked in the first paper that we reviewed.
It has not been until recently that the use of TXA in traumatic brain injury (TBI) has been studied. We know that severe TBI is a leading cause of trauma-related mortality and disability worldwide.[4] We also know that severe TBI is commonly associated with the development of intracranial hemorrhage where the presence and volume of blood are associated with increased mortality and poor outcomes.[5] One would then surmise that the use of TXA in patients with TBI would prevent the progression to severe TBI and subsequent morbidity and mortality. We review two articles which address this very question.
Lastly, the use of TXA is not without risk. We know that if administered too rapidly, it can lead to hypotension and other adverse effects including seizures, headaches, backache, abdominal pain, nausea, vomiting, diarrhea, fatigue, pulmonary embolism, deep vein thrombosis, anaphylaxis, impaired color vision, and other visual disturbances.[1] Notable here are the risks of pulmonary embolism and deep vein thrombosis. While TXA is an antifibrinolytic and not a procoagulant, studies have demonstrated associations of thrombotic events in those treated with TXA (though not always statistically significant and no causation has been proven). In the last study we review the incidence of venous thromboembolic events in trauma patients who have received TXA.
Articles reviewed
1. Guyette FX, Brown JB, Zenati MS, et al. Tranexamic acid during prehospital transport in patients at risk for hemorrhage after Injury: a double-blind, placebo-controlled, randomized clinical trial. JAMA Surg.2021;156(1):11–20. [Pubmed]
2. The CRASH-3 trial collaborators. Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities on patients with acute traumatic brain injury (CRASH-3): a randomized, placebo-controlled trial. Lancet 2019; Vol 394, Iss 10210, P 1713-1723[Full Text].
3. Bossers SM, Loer SA, Bloemers FW, et al. Association between prehospital tranexamic acid administration and outcomes of severe traumatic brain injury. JAMA Neurol. 2021;78(3):338–345. [Pubmed]
supplemental reading
4. Rivas L, Estroff J, Sparks A, et al. The incidence of venous thromboembolic events in trauma patients after tranexamic acid administration: an EAST multicenter study. Blood Coagul Fibrinolysis. 2021 Jan 1;32(1):37-43. [Pubmed]
DOES PRESHOSPITAL TXA OFFER MORTALITY BENEFIT? - GUYETTE ET AL
This phase 3 multicenter double-blind, placebo-controlled randomized clinical trial looked at the prehospital safety and efficacy of prehospital TXA administration. The investigators hypothesized that prehospital administration of TXA would improve 30-day mortality in eligible trauma patients.
Four level-1 US trauma centers participated in the study where the inclusion criteria were trauma patients who were within 2 hours of their injury and were transported to the trauma center from either the field or another hospital. Trauma patients between the ages of 18-90 years had to have either had one documented episode of hypotension (defined as a systolic BP <90 mmHg) or tachycardia (>100 beats/minute) to be included in the study. Patients were excluded if they did not have IV/IO access, mechanism was a simple fall from standing, they had a c-spine injury, suffered a traumatic arrest of > 5 minutes, suffered penetrating brain injury, drowning, hanging, were pregnant, were a prisoner, had an opt-out bracelet or declined to be in the study.
Patients received either 1g of TXA or placebo in the prehospital setting. Those that received TXA were broken up into 3 treatment arms: no further TXA, in-hospital 1g TXA infusion, or in-hospital 1g bolus followed by a 1g infusion (see Figure 1). The primary outcome was 30-day mortality with secondary outcomes looking at 24 hour in-hospital mortality, blood resuscitation at 6 and 24 hours, incidence of multiorgan failure, ARDS, nosocomial infection, early seizures, PE/DVT, crystalloid resuscitation after 24 hours, and the incidence of coagulopathy. A total of 927 patients were enrolled with ultimately 447 in the TXA arm and 456 in the placebo arm after withdrawals or ineligibilities. There was a median injury severity score of 12 with an all-cause mortality of 9%.


Kaplan-Meier estimates of 30-day survival rate among patients randomzied to the prehospital tranexamic acid or placebo intervention.
This study found that the 30-day mortality was 8.1% in the TXA group and 9.9% in the placebo group which was not statistically significant (see Table 2). There were no differences found in the secondary outcomes. In further analysis, they found no difference in the number of arterial thrombotic complications (i.e. MI or stroke). A post-hoc analysis showed a lower 30-day mortality of those receiving TXA within an hour of their injury. When looking at the subgroups with severe shock, there was an 18.5% mortality in the TXA group vs. 35% in placebo, though the study was not powered in these subgroups to deem whether or not this was statistically significant. This study was stopped early (at 93% of planned enrollment) and therefore underpowered, particularly for the secondary outcomes.
Limitations of this study were that there were overall low injury severity scores and transfusion requirements which introduces a potential bias. One also has to keep in mind that this study occurred at Level 1 trauma centers and may not be applicable in critical access hospitals or lower leveled trauma centers.
Bottom Line: There does not appear to be a 30 day mortality benefit for trauma patients given TXA pre-hospital (vs in- hospital). When stratifying TXA administration time after injury and qualifying shock incidence, there appeared to be a lower 30 d mortality if TXA was given within 1 hour of the incident.
DOES TXA IMPROVE OUTCOMES IN PATIENTS WITH TBI? - CRASH-3 TRIAL COLLABORATORS
This international, multi-center, randomized, placebo-controlled trial looked at the effects of TXA on head injury-related death, disability, and adverse events in adult patients with TBI.
Inclusion criteria included adults who were within 3 hours of injury, had a GCS of < 13 or any intracranial bleeding on CT, and no major extracranial bleeding. The placebo group received a bolus of saline followed by an 8-hour infusion of saline whereas the study group received a 1 g loading dose of TXA over 10 minutes followed by 1 gram infusion over 8 hours. The primary outcome was head injury-related death in-hospital within 28 days of injury. Secondary outcomes were early head injury related death (within 24 hours after injury), all-cause and cause-specific mortality, disability, vascular occlusive events (MI, stroke, DVT, PE), seizures, complications, neurosurgery, days of ICU care, and adverse events within 28 days.
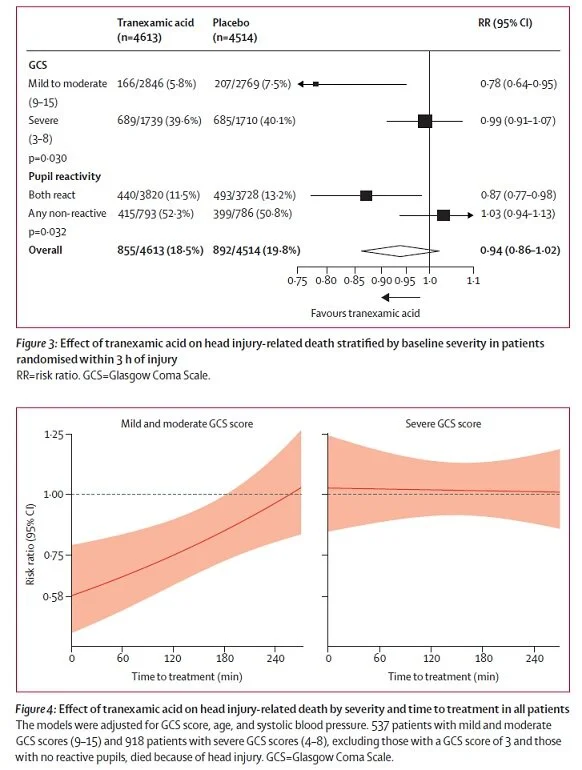
The authors found a reduction in the risk of head injury-related deaths with TXA in a subgroup of patients with mild-to-moderate head injury, but in patients with severe injury, no clear evidence of reduction was noted. The prevalence of disability among the survivors of the two groups was similar. The authors concluded that the administration of TXA to patients with TBI within 3 hours of injury reduces head injury-related death, with no evidence of adverse effects or complications. They also state that the effect of tranexamic acid on head injury-related death appeared to depend on the time interval between injury and the initiation of the trial treatment and on the severity of TBI with early treatment of patients with mild and moderate head injury conferring the greatest mortality benefit. They surmised that patients with severe head injury might have had less to gain from TXA than patients with mild-to-moderate head injury. Secondary outcome analysis showed that the risk of vascular occlusive events was similar between the two groups.
This was an impressive study and one that we have all been waiting for. At first glance, this seems like we have our answer. However, it should be noted that this study was underpowered as they had to change inclusion criteria part way through after the publication of CRASH-2 and the WOMAN trials noted no significant effect of TXA if given > 3 hours from time of injury.[8] When looking at their primary outcome, there was NO statistical significance of head-injury related death between the two groups at 28 days. Mortality was unchanged, disability was unchanged. In the subgroup analysis where they looked at the mild-to-moderate TBI patients, they did not report the all-cause mortality.
Bottom line: Though we were hoping for TXA to be a wonder drug for our TBI patients, it appeared to confer no mortality benefit at 28 days. The next study, however, shows that it might actually be associated with harm in the isolated TBI patient.
DOES TXA IMPROVE OUTCOMES IN PATIENTS WITH TBI? - BOSSERS ET AL
This was a retrospective cohort study of the prospectively collected observational data from the BRAIN-PROJECT.[9] The BRAIN-PROJECT was a multicenter observational study of the prehospital treatment of patients with severe TBI (based on trauma mechanism or clinical findings and a prehospital GCS <9) who were treated by one of the four Dutch physician-staffed Helicopter Emergency Medical Services from 2012-2017.
Inclusion was based on suspected rather than confirmed TBI given treatment was in the field. Patients were excluded if they were not transported to a participating trauma center or had cardiopulmonary arrest. The primary outcome was 30-day mortality with secondary outcomes of 1-year functional neurological outcome based on GCS as well as hospital length of stay.
Within the database of the 2589 patients transported, 1375 had confirmed TBI, of which 719 were isolated TBI. A total of 693 patients received prehospital TXA (90% received 1 gram, 4 patients received more than 2g of TXA). The authors looked at three study groups: a) full cohort, b) patient with confirmed TBI (Head Abbreviated Injury Score [AIS] was >2), c) patients with isolated TBI (Head AIS of >2 with other body area injury scores of <3). They found that of the three cohorts, after adjusting for confounders, that there was no evidence of increased survival in the full cohort and in the patients with confirmed TBI who received TXA. However, in patients with isolated TBI, there was a substantially increased odds of mortality with an OR of 4.45.

Bottom line: In this limited retrospective cohort study, that there was no evidence of increased survival in the full cohort and in the patients with confirmed TBI who received TXA.
IS THERE A HIGHER RATE OF THROMBEMBOLIC EVENTS IN PATIENTS GIVEN TXA? - RIVAS ET AL
This multicenter retrospective review sought to evaluate the incidence of VTE, CVA, and MI in bleeding, injured patients who received TXA in their initial resuscitation vs. those who did not.
Injured patients between 18-80 years of age who presented directly to a level-1 or level-2 trauma center from the scene and received at least 5 units of PRBC within the first 24 hours were included in this study. Patients were excluded if they died within 24 hours of arrival, were pregnant, received TXA more than 3 hours after the injury or lacked documentation regarding the timing of TXA administration. If the trauma center performed screening ultrasounds to evaluate for asymptomatic DVTs, they were not included in this study. A total of 1333 patients across 17 trauma centers were enrolled. 67% received TXA. There was no difference in the associated risk of VTE or MI/CVA after multivariable risk adjustment. Additional findings demonstrated that the group who received TXA, received up to 30% less blood products in the first 24 hours and that hospital mortality was lower in the TXA group.

Bottom Line: This is yet another study that demonstrates the lack of significant venous thromboembolic events or arterial thromboembolic events in trauma patients who received TXA.

TXA can be administered safely in the prehospital setting to patients who have traumatic injuries and demonstrate hemodynamic instability.
The benefits from TXA appear to be associated with earlier administration.
Further studies need to be performed to determine the best TXA dosing regimen.
The use of TXA in isolated head trauma does not change the 28-day mortality rate and may actually be harmful in isolated TBI patients.
TXA does not increase the incidence of thromboembolic events such as DVT/PE, stroke, or MI.
Download article summaries

GUYETTE ET AL

Bossers ET AL

RIVAS ET AL
Authored by Kate Zimmerman DO, Katie Main MD, and Rebecca Bloch MD
Edited and Posted by Jeffrey A. Holmes, MD
References
Nishida T, Kinoshita T, Yamakawa K. Tranexamic acid and trauma-induced coagulopathy: the past, present, and future. J Thromb Haemost 2019;17:852-862.[Pubmed]
Morrison JJ, Dubose JJ, Rasmussen TE et al. Military application of tranexamic acid in trauma emergency resuscitation (MATTERs)study. Arch Surg 2012; 147:113-119.[Pubmed]
CRASH-2 Study Collaborators. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant hemorrhage (CRASH-2): a randomized, placebo-controlled trial. Lancet 2010; 376:23-32.[Pdf]
Rubiano AM, Carney N, Chestnut R et al. Global neurotrauma research challenges and opportunities. Nature. 2015;527(7578):s193-197.
Perel P, Roberts I, Bouamra O et al. Intracranial bleeding in patients with traumatic brain injury: a prognostic study. BMC Emerg Med. 2009;9:15 [Pubmed]
Calculated Decisions - Injury Severity Score [Pdf].
WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomized, double-blind, placebo-controlled trial. Lancet 2017;389:2105-16.[Pdf]
Bossers SM, Boer C, Greuters S, et al; BRAIN-PROJECT collaborators. Dutch prospective observational study on prehospital treatment of severe traumatic brain injury: the BRAIN-PROJECT study protocol. Prehosp Emerg Care. 2019;23(6):820-827.[Full Text]







